
Hemorrhoids
Hemorrhoids are when the veins or blood vessels in and around your anus and lower rectum become swollen and irritated. This happens when there is extra pressure on these veins.
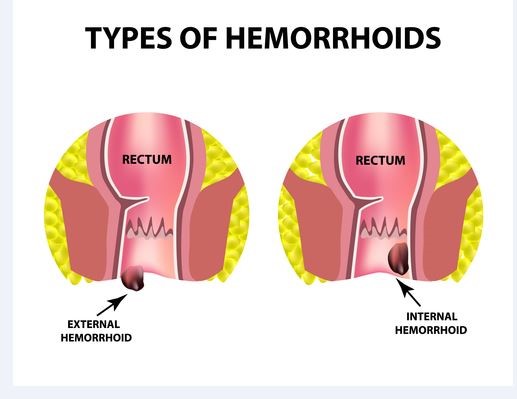
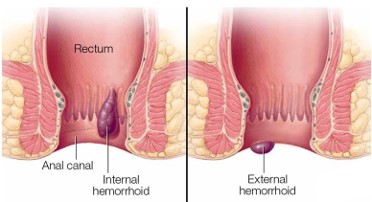
Hemorrhoids can be either inside your anus (internal) or under the skin around your anus (external).
They are very common in both men and women. About half of all people will have hemorrhoids by age 50.
Many women get hemorrhoids during pregnancy and childbirth. The pressure of carrying a baby in your belly puts extra stress on the blood vessels in your pelvic area. Straining to push the baby out when giving birth also puts extra pressure on these blood vessels.
Hemorrhoidal disease is ranked first amongst diseases of the rectum and large intestine, and the estimated worldwide prevalence ranges from 2.9% to 27.9%, of which more than 4% are symptomatic (1, 2). Approximately, one third of these patients seek physicians for advice. Age distribution demonstrates a Gaussian distribution with a peak incidence between 45 and 65 years with subsequent decline after 65 years (3, 4). Men are more frequently affected than women
Laser Hemorrhoidoplasty Procedure vs Open Surgical Hemorrhoidectomy: a Trial Comparing 2 Treatments for Hemorrhoids of Third and Fourth Degree

What Causes Hemorrhoids?
Hemorrhoids are swollen veins in the lowest part of your rectum and anus. They occur when the blood vessel walls stretch and thin and allow the veins to bulge and become irritated. Internal hemorrhoids usually cannot be seen, as they are far inside the rectum. The only way a person knows they have them is from bleeding. External hemorrhoids are under the skin around the anus. Due to the many nerves in this area, external hemorrhoids usually hurt.
There is a genetic predisposition toward getting hemorrhoids. Basically, hemorrhoids develop when there is a buildup of pressure in the lower rectum that affects blood flow, making the veins in the area swell. There are various reasons this happens:
- Obesity
- Pregnancy
- Pushing during bowel movements
- Straining such as during heavy lifting
- Standing or sitting for long stretches
- Lasting constipation or diarrhea
- You may get hemorrhoids if you:
- Often strain during bowel movements
- Pregnant
- Have a family history of hemorrhoids
- Old
- Have long-term or chronic constipation or diarrhea
Who is at risk for hemorrhoids?
- Hemorrhoids are very common. Most people will have a hemorrhoid at some time in their life.
You are more likely to get hemorrhoids if you:
- Are pregnant
- Sit on the toilet for too long
- Are obese
- Do things that make you strain more, such as heavy lifting
- Have a family history of hemorrhoids
- Have long-term or chronic constipation or diarrhea
- Are between 45 and 65 years old
- What are the symptoms of hemorrhoids?
- Each person’s symptoms may vary. Some of the most common symptoms include:
- Bright red blood in your stool, on toilet paper, or in your toilet bowl
- Pain and irritation around your anus
- Swelling or a hard lump around your anus
- Itching
How are hemorrhoids diagnosed?
Having blood in your stool can also be a sign of other digestive disorders, such as colorectal cancer. It’s important to see your healthcare provider for a complete exam.
To see if you have hemorrhoids, your healthcare provider may do several tests including:
Physical exam. This is done to check your anus and rectum and look for swollen blood vessels that are a sign of hemorrhoids.
Digital rectal exam (DRE). Your healthcare provider inserts a gloved, greased (lubricated) finger into your rectum to check for any problems.
Anoscopy. A hollow, lighted tube is put into your anus. This is used to see internal hemorrhoids.
Proctoscopy. A lighted tube is put into your anus. This gives a view of your entire rectum.
Sigmoidoscopy. This test checks the inside of part of your large intestine. It helps to tell what is causing diarrhea, belly pain, constipation, abnormal growths, and bleeding. A short, flexible, lighted tube (sigmoidoscope) is put into your intestine through the rectum. This tube blows air into your intestine to make it swell. This makes it easier to see inside. A tissue sample (biopsy) can be taken if needed.
Colonoscopy. This test looks at the full length of your large intestine. It can help check for any abnormal growths, tissue that is red or swollen, sores (ulcers), or bleeding. A long, flexible, lighted tube called a colonoscope is put into your rectum up into the colon. This tube lets your healthcare provider see the lining of your colon and take out a tissue sample (biopsy) to test it. He or she may also be able to treat some problems that may be found.
Classification of Piles
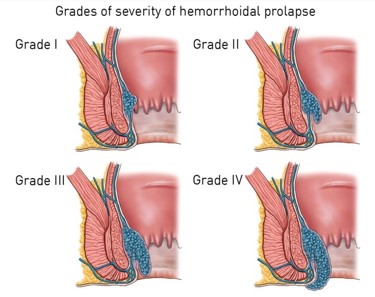
Piles may be internal or external. Internal piles are further classified into grades:
Grade I – No protrusion from anus.
Grade II – Protrusion through the anus during straining and defecation, but return spontaneously.
Grade III – Protrude through the anus with defecation or straining, but manually reduced.
Grade IV – Protrude and cannot be manually reduced.
How are hemorrhoids treated?
Treatment will depend on your symptoms, age, and general health. It will also depend on how severe the condition is.
The main goal of treatment is to reduce your symptoms. This may be done by:
Sitting in plain, warm water in a bathtub several times a day
Using ice packs to reduce swelling
Using hemorrhoid creams or medicines inserted into your rectum (suppositories)
Your healthcare provider may also suggest that you add more fiber and fluids to your diet to help soften your stools. Having softer stools means you don’t have to strain during bowel movements. This reduces the pressure on your hemorrhoids.
- Adding more fiber to your diet means eating more:
- Fruits
- Vegetables
- Whole grains
- Your healthcare provider may also suggest that you take stool softeners or fiber supplements.
The treatment options for symptomatic hemorrhoids have varied over time. Measures have included conservative medical management, non-surgical treatments and various surgical techniques. The various non-surgical treatments include rubber band ligation (RBL), injection sclerotherapy, cryotherapy, infrared coagulation, laser therapy and diathermy coagulation; all of which may be performed as out patient procedures without anaesthesia. These nonsurgical methods are considered to be the primary option for grades one to three (grade I-III) hemorrhoids (8). If conservative measures fail to control symptoms, patients may be referred to a surgeon for operative management. The indications for the surgical treatment include the presence of a significant external component, hypertrophied papillae, associated fissure, extensive thrombosis or recurrence of symptoms after repeated RBL.
In some cases, surgery is needed. There are several types of surgeries used to remove or reduce internal and external hemorrhoids. These include:
Rubber band ligation. A rubber band is placed around the base of the hemorrhoid inside your rectum to cut off circulation to the hemorrhoid. The hemorrhoid shrinks and goes away in a few days.
Sclerotherapy. A chemical solution is shot (injected) around the blood vessel to shrink the hemorrhoid.
Electrical coagulation, also called infrared photo coagulation. A special device uses a beam of infrared light to burn hemorrhoid tissue.
Hemorrhoidectomy and hemorrhoidopexy. These procedures permanently remove your hemorrhoids.
What are possible complications of hemorrhoids?
In rare cases, hemorrhoids may cause other problems. These may include:
Having a low blood count that makes you tired (anemia). This can happen because of bleeding from a long-term or chronic hemorrhoid.
Blood flow being cut off from a hemorrhoid that is sticking out (prolapsed). This can happen when the blood supply to the hemorrhoid is cut off. This can be very painful and cause bleeding. You may need surgery.
The technique employed may be open (Milligan–Morgan) or closed (Ferguson) and the instruments used are scalpel, scissor, electrocautery or laser. Milligan-Morgan hemorrhoidectomy is the gold standard and frequently performed procedure in the United Kingdom (9). Post hemorrhoidectomy pain is the commonest problem associated with the surgical techniques. The other early complications are urinary retention (20.1%), bleeding (secondary or reactionary) (2.4%–6%) and subcutaneous abscess (0.5%). The long-term complications include anal fissure (1% -2.6%), anal stenosis (1%), incontinence (0.4%), fistula (0.5%) and recurrence of hemorrhoids (10, 11).
What can I do to prevent hemorrhoids?
It’s not always possible to stop hemorrhoids from happening. But you may reduce your risk of getting hemorrhoids if you:
- Eat a healthy diet, with plenty of fiber and liquids.
- Limit the amount of time you sit on the toilet.
- Work with your healthcare provider to manage constipation and prevent straining.
- Stay at a healthy weight.
When should I call my healthcare provider?
Call your healthcare provider if your symptoms get worse or if you notice any new symptoms. Also call if you see blood in your stool or on toilet paper for the first time, or if you see more blood than normal.
Key points about hemorrhoids
Hemorrhoids are a swelling of the veins or blood vessels in and around your anus and lower rectum. This happens when there is extra pressure on these veins.
Hemorrhoids are either inside your anus (internal) or under the skin around your anus (external).
About half of all people will have hemorrhoids by age 50.
Many women get hemorrhoids during pregnancy and childbirth.
You may get hemorrhoids if you have a family history, often strain during bowel movements, or have long-term (chronic) constipation or diarrhea.
Symptoms may include blood in your stool, pain around your anus, or itching.
Your healthcare provider may do several tests to be sure you have hemorrhoids.
You may need to add more fiber and fluids to your diet.
The goal of treatment is to reduce your symptoms.
In some cases, surgery is needed.
What is pilonidal sinus disease (PNS)?
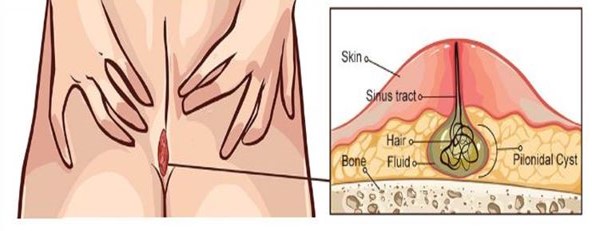

A pilonidal sinus (PNS) is a small hole or tunnel in the skin. It may fill with fluid or pus, causing the formation of a cyst or abscess. It occurs in the cleft at the top of the buttocks. A pilonidal cyst usually contains hair, dirt, and debris. It can cause severe pain and can often become infected. If it becomes infected, it may ooze pus and blood and have a foul odor.
A PNS is a condition that mostly affects men and is also common in young adults. It’s also more common in people who sit a lot, like cab drivers.
What are the causes of pilonidal sinus disease?
- The exact cause of this condition isn’t known, but its cause is believed to be a combination of changing hormones (because it occurs after puberty), hair growth, and friction from clothes or from spending a long time sitting.
- Activities that cause friction, like sitting, can force the hair growing in the area to burrow back under the skin. The body considers this hair foreign and launches an immune response against it, similar to how it would react when dealing with a splinter. This immune response forms the cyst around your hair.
- Sometimes a person may have multiple sinuses that connect under the skin that is expressed by multiple openings on external skin.
Identifying a pilonidal sinus and recognizing signs of infection
You may not have any noticeable symptoms at first other than a small, dimple-like depression on the surface of your skin. However, once the depression becomes infected, it will quickly develop into a cyst (a closed sac filled with fluid) or an abscess (a swollen and inflamed tissue where pus collects).
The signs of an infection include:
- pain when sitting or standing
- swelling of the cyst
- reddened, sore skin around the area
- pus or blood draining from the abscess, causing a foul odor
- hair protruding from the lesion
- formation of more than one sinus tract, or holes in the skin
- You may also experience a low-grade fever, but this is much less common.
How are pilonidal sinuses treated?
- Conservative treatment
If your case is diagnosed early on, you aren’t experiencing severe pain, and there’s no sign of inflammation, it’s likely that your doctor will prescribe a broad-spectrum antibiotic. A broad-spectrum antibiotic is an antibiotic that treats a wide range of bacteria. It’s important to realize that this won’t heal the sinus tract, but it will give you relief from the infection and discomfort. Your doctor will recommend that you get a follow-up exam, regularly remove hair or shave the site, and pay particular attention to hygiene.
- Lancing (I&D)
This procedure alleviates symptoms from an abscess, or a collection of pus inside the sinus. Before this procedure, your doctor will give you a local anesthetic. They will then use a scalpel to open the abscess. They will clean away any hair, blood, and pus from inside the abscess.
Your doctor will pack the wound with sterile dressing and allow it to heal from the inside out. The wound usually heals within four weeks, and many people don’t require any further treatment.
- Phenol injection
For this type of treatment, your doctor will first give you a local anesthetic. They will then inject phenol, a chemical compound used as an antiseptic, into the cyst. This procedure may need to be repeated several times. Eventually, this treatment will cause the lesion to harden and close.
This treatment has a very high recurrence rate. Therefore, it’s uncommon in the United States. Doctors turn to surgery as the treatment of choice in these cases.
- Surgery
If you have a recurring PNS or if you have more than one sinus tract, your doctor will recommend a surgical procedure.
You will first be given a local anesthetic (preferably general anasthesia). Then, the surgeon will open the lesions, removing all of the pus and debris. Once this process is complete, the surgeon will stitch the wounds closed.
After surgery, your doctor will explain how to change the dressings and will recommend shaving the site to prevent hair from growing into the wound.
What is the outlook for pilonidal sinus disease?
Depending on the severity of the disorder and the type of treatment, a PNS will usually clear up within 4 to 10 weeks.
What complications are associated with pilonidal sinus disease?
There are a number of complications that may arise from PNS. These include wound infection and a recurrence of the PNS even after surgery.
Signs that the wound is infected include:
- severe pain
- inflamed, swollen skin
- a temperature of 38 °C or higher
- blood and pus seeping from the wound site
- a foul odor coming from the wound
How can I prevent pilonidal sinus disease?
- You can prevent recurrence of PNS by washing the area on a daily basis with a mild soap, making sure all soap is removed, keeping the area completely dry, and avoiding sitting for long periods.
