Gynecomastia
Gynecomastia is a benign enlargement of the male breast resulting from a proliferation of the glandular component of the breast (see the image below). Gynecomastia is defined clinically by the presence of a rubbery or firm mass extending concentrically from the nipples. Although the condition is usually bilateral, it can be unilateral. The condition known as pseudogynecomastia, or lipomastia, is characterized by fat deposition without glandular proliferation.
Gynecomastia can be physiologic or pathologic. Physiologic gynecomastia is seen in newborn infants, pubescent adolescents, and elderly individuals

Causes
Gynecomastia is thought to be caused by an altered ratio of estrogens to androgens mediated by an increase in estrogen production, a decrease in androgen production, or a combination of these two factors.Estrogen acts as a growth hormone to increase the size of male breast tissue. The cause of gynecomastia is unknown in around 25% of cases.Drugs are estimated to cause 10–25% of cases of gynecomastia.
Certain health problems in men such as liver disease, kidney failure, or low testosterone can cause breast growth in men.
Physiologic
Both male and female newborns may show breast development at birth or in the first weeks of life.
Gynecomastia in adolescents usually starts between the ages of 10 and 12 and commonly goes away after 18 months.
Declining testosterone levels and an increase in the level of subcutaneous fatty tissue seen as part of the normal aging process can lead to gynecomastia in older men. known as senile gynecomastia.
Non-physiologic:
- Medicines
- Chronic disease
- kidney failure
- liver failure or cirrhosis.
- Hyperthyroidism
- Malnutrition:
- Tumors
- Drugs:Antiandrogen/inhibitors of androgen synthesis are as follows: Flutamide, Ketoconazole,Spironolactone
Cancer/chemotherapeutic drugs are as follows: Alkylating agents, Methotrexate,Vinca alkaloids, Imatinib
Cardiac and antihypertensive medications are as follows: Calcium channel blockers (verapamil, nifedipine, diltiazem)
ACE Inhibitors (captopril, enalapril)
Digoxin, Alpha-blockers, Amiodarone
Hormones are as follows: Androgens, Anabolic steroids, Estrogens, Growth hormones, Chorionic gonadotropin
Psychoactive drugs are as follows: Diazepam, Tricyclic antidepressants, Haloperidol
Drugs for infectious diseases are as follows: Antiretroviral therapy for HIV/AIDS (eg, indinavir), Isoniazid, Ethionamide, Metronidazole, Ketoconazole
Drugs of abuse are as follows: Amphetamines, Heroin, Methadone, Alcohol, Marijuana
Others are as follows: Theophylline, Omeprazole, Domperidone, Penicillamine, Heparin, Methotrexate
Drugs can also be stratified depending on the evidence that supports their association with gynecomastia, as follows:
Probable – Estrogenlike or estrogen receptor binders, verapamil, spironolactone, cimetidine and ketoconazole
Possible – Digoxin , nifedipine, cytotoxic agents, and marijuana
Uncertain– alfa-blockers, and diazepam
Signs and symptoms
A thorough history should be obtained that addresses the following:
- Age of onset and duration of the condition
- Any recent changes in nipple size and any pain or discharge from the nipples
- History of mumps, testicular trauma, alcohol use, or drug use
- Family history of gynecomastia
- History of sexual dysfunction, infertility, or hypogonadism
Estimates suggest the following etiologies in males seeking medical attention for gynecomastia:
- Persistent pubertal gynecomastia – 25%
- Drugs – 10-25%
- No detectable abnormality – 25%
- Cirrhosis or malnutrition – 8%
- Primary hypogonadism – 8%
- Testicular tumors – 3%
- Secondary hypogonadism – 2%
- Hyperthyroidism – 1.5%
- Chronic renal insufficiency – 1%
Physical examination should include the following:
- Thorough examination of the breasts, with attention to size and consistency
- Assessment for any nipple discharge or axillary lymphadenopathy
- Testing to differentiate between true gynecomastia and pseudogynecomastia
- Assessment of glandular tissue
- Examination of the testicles, with attention to size and consistency, as well as nodules or asymmetry
- Observation of any signs of feminization
- Checking for any stigmata of chronic liver disease, thyroid disease, or renal disease
Diagnosis
Patients with physiologic gynecomastia do not require further evaluation. Similarly, asymptomatic and pubertal gynecomastia do not require further tests and should be reevaluated in 6 months. Further evaluation is necessary in the following situations:
Breast size greater than 5 cm (macromastia)
A lump that is tender, of recent onset, progressive, or of unknown duration
Signs of malignancy (eg, hard or fixed lymph nodes or positive lymph node findings)
Laboratory tests that may be considered include the following:
- Serum chemistry panel
- Free and total testosterone, luteinizing hormone (LH), estradiol, and dehydroepiandrosterone sulfate levels (DHEA)
- Thyroid-stimulating hormone (TSH) and free thyroxine levels
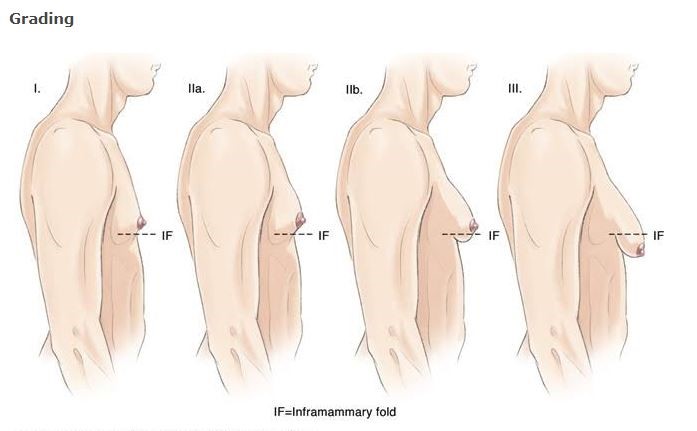
Classification
The spectrum of gynecomastia severity has been categorized into a grading system:
- Grade I: Minor enlargement, no skin excess
- Grade II: Moderate enlargement, no skin excess
- Grade III: Moderate enlargement, skin excess
- Grade IV: Marked enlargement, skin excess
Imaging studies that may be helpful include the following:
Mammography: Indicated if one or more features of breast cancer are apparent upon clinical examination, [1] followed by fine-needle aspiration or breast biopsy as appropriate [2, 3]
Testicular ultrasonography: Indicated if the serum estradiol level is elevated and the clinical examination findings suggest the possibility of a testicular neoplasm
Breast ultrasonography (though the positive predictive value of imaging in males is low [4] )
CT: Gynecomastia is often reported on CT scans
Treatment
General treatment considerations are as follows:
As a rule, no treatment is required for physiologic gynecomastia
Pubertal gynecomastia resolves spontaneously within several weeks to 3 years in most patients; breasts larger than 4 cm in diameter may not regress completely
Identifying and managing an underlying primary disorder often alleviates breast enlargement
For patients with idiopathic gynecomastia or with residual gynecomastia after treatment of the primary cause, medical or surgical treatment may be considered.
If medical therapies are used, they should be tried early in the condition’s course
Pharmacologic agents used to treat gynecomastia include the following:
- Clomiphene
- Tamoxifen
- Danazol (less frequently used)
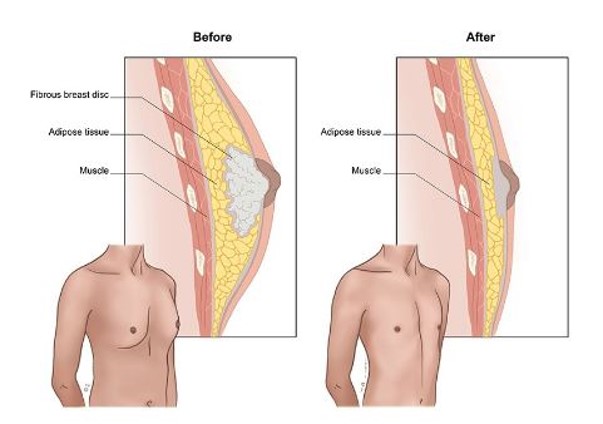
Surgical approaches that may be considered include the following:
- Reduction mammoplasty: Considered in cases of macromastia, long-standing gynecomastia, or failed medical therapy, as well as for cosmetic reasons
- More extensive plastic surgery: May be considered in cases of marked gynecomastia or excessive sagging of the breast tissue from weight loss, in some cases, the surgical procedure might necessitate to add liposuction procedure to get a satisfactory result.
Surgical complications may include the following:
- Sloughing of tissue due to a compromised blood supply
- Contour irregularity
- Hematoma or seroma formation
- Permanent or partial numbness in the nipple-areolar area
